
SAMPLE QUESTIONS TAKEN FROM CURRENT USMCP QBANK FOR STEP 2 CK
Current projects:
1. USMCP Step 2 CK Qbank = Active
2. USMCP Step 2 CK Self Assessment Exam Form 1 = DONE
3. USMCP Step 1 Qbank = Active
4. USMCP Step 1 self Assessment Exam Form 2 = Active
Email us if interested in joining the team to write questions: This email address is being protected from spambots. You need JavaScript enabled to view it.
STEP 2 qbank EXAMPLES:
Pediatrics - Pulmonary
by
(Dr. Swanand Rewatkar - USMCP TEAM)
18 months old girl brought by father in the clinic with c/o increasing cough, fever and runny nose since last 3 days. It started with fever before 3 days. The fever was mild to moderate with the thermometer reading of 38.5 to 390C and was responding to the paracetamol. According to him mother gave her paracetamol approximately 2 times daily with a gap of 12 hours. Father told that she also has runny nose with mucoid secretions for the same duration. She developed cough yesterday morning and it is increasing gradually since then. She was coughing a lot last night that kept her awake for the whole night. Since morning the cough has become more louder like dog barking and more frequent that made him bring the child to the clinic. She is taking her feeds well and passing urine 4 to 6 times a day. She is playful but with cough she is becoming irritable. She was born by LSCS at 37 weeks of gestation as mother had preeclampsia. APGAR was 9 and 10 at 1 and 5 min respectively. No history of NICU stay. She was breastfed for 6 months and then started on the complementary feeds. Now she is accepting the food from the family pot. Her milestones are appropriate for her age and anthropometrically she is at 50th percentile on growth charts. O/E She is sitting comfortably in father’s lap, HR -110/min, RR- 32/min, CRT <2 sec, NO cyanosis, LNpathy, no signs of respiratory distress, SPo2- 96%, no rash, Temp- 38.7OC, RS- Air entry bilaterally +nt, Inspiratory stridor heard all over the chest during auscultation, CVS- S1S2 nl, no murmur, Abdomen- soft non-tender, Liver 1 cm Palpable no splenomegaly. The stridor was audible as she started crying while examining her.
What should be the treatment plan for this child?
A. A. Start on the paracetamol PRN, adequate hydration, penicillin V po, follow up in 3 days
B. B. Send CBC, CRP, urine r/m, nasal swab for H1N1, follow up with result
C. C. Start on the paracetamol and oral hydration, follow up after 2 days
D. D. Start PO steroid, paracetamol prn, advice for hydration and follow up advice.
E. E. Send her to emergency for the opinion of paediatric respiratory specialist.
EXPLANATION: The Correct Answer is D
This child is suffering from mild to moderate croup, the most common form of acute upper respiratory obstructive diseases. Viruses typically cause croup, the parainfluenza viruses (types 1, 2, and 3); account for approximately 75% of cases; other viruses associated with croup include influenza A and B, adenovirus, respiratory Syncytial virus, and measles.
Most patients have an upper respiratory tract infection with combination of rhinorrhea, pharyngitis, mild cough, and low-grade fever for 1-3 days before the signs and symptoms of upper airway obstruction become apparent. The child then develops the characteristic “barking” cough, hoarseness, and inspiratory stridor. Symptoms are characteristically worse at night and often recur with decreasing intensity for several days and resolve completely within a week. Agitation and crying greatly aggravate the symptoms and signs. Physical examination can reveal a hoarse voice, coryza, normal to moderately inflamed pharynx, and a slightly increased respiratory rate. Patients vary substantially in their degrees of respiratory distress. Rarely, the upper airway obstruction progresses and is accompanied by an increasing respiratory rate; nasal flaring; suprasternal, infra-sternal, and intercostal retractions; and continuous stridor. Croup is a disease of the upper airway, and alveolar gas exchange is usually normal. Hypoxia and low oxygen saturation are seen only when complete airway obstruction is imminent. The child who is hypoxic, cyanotic, pale, or obtunded needs immediate airway management. Croup is a clinical diagnosis and does not require a radiograph of the neck. Radiographs of the neck can show the typical subglottic narrowing, or steeple sign, of croup on the postero-anterior view.
The mainstay of treatment for children with croup is airway management and treatment of hypoxia. Oral corticosteroid is the drug of choice for croup. oral dexamethasone used as a single dose of 0.6 mg/ kg, a dose as low as 0.15 mg/kg may be just as effective. Intramuscular dexamethasone and nebulized budesonide have an equivalent clinical effect; oral dosing of dexamethasone is as effective as intramuscular administration. Most children with either acute spasmodic croup or infectious croup can be managed safely at home.
Nebulized racemic epinephrine is an accepted treatment for moderate or severe croup. The indications for the administration of nebulized epinephrine include moderate to severe stridor at rest, the possible need for intubation, respiratory distress, and hypoxia.
Option D.- Shows the most correct regimen for the treatment of croup from the available option. Hence other options are incorrect.
Education Objective:
Croup is the most common form of acute upper respiratory obstruction in infancy. Most children with either acute spasmodic croup or infectious croup can be managed safely at home. Oral corticosteroid is the drug of choice for croup. Nebulized racemic epinephrine is an accepted treatment for moderate or severe croup.
Gastrointestinal - Choledochal Cyst
A 28 year old Japanese female presents to the ER writhing with pain in the right upper abdomen radiating to the back associated with high grade fever. On physical examination, her vitals were as follows: PR=95/min, BP=130/90, RR=26/min, Temperature= 103.6oF. She has vomited twice in the ER within a span of half an hour. On abdominal examination, tenderness along with rigidity was found. A mass was found per abdomen to the right and above the umbilicus, smooth, soft, not moving with respiration and not mobile. Her eyes and skin were found to be yellow. She was started on IV ringer lactate and pethidine with ondansetron. An ultrasound was done which revealed cystic dilatation of intraduodenal part of CBD. Blood work showed: WBCs: 17x109/L, LDH: 750 units/L, Blood glucose: 11mmol/L, S. Bilirubin: 4 mg/dl.
She was immediately admitted to the ICU and the initial treatment was continued. What is the next step in management of this patient?
-
Monitoring of vitals, CVP and urine output along with supplemental O2
-
IV imipenem and ranitidine
-
Nasogastric tube for TPN
-
Endoscopic Sphincterotomy
-
Urgent ERCP
EXPLANATION: The Correct Answer is A
Choledochal cyst defined as an isolated/focal or combined/diffuse congenital dilatation of extra or intrahepatic biliary tree. It is a congenital cyst with partial or complete weakness of the common Bile Duct (CBD) biliary wall. It may be single/multiple or extrahepatic or intrahepatic. It is more common in Asia, moslty in Japan, incidence is 1 in 1000. It is often associated with pancreaticobiliary maljunction. There is long common channel more than 2 cm. It causes reflux of pancreatic juice into the bile duct, enzymatic destruction of the bile duct wall, ductal wall weakening and dilatation—Babbit theory.( Riya Kaur Kalra- USMCP TEAM)
|
Types of Choledochal Cysts (Todani Modifications Of Alonso-Lej Classification) |
|
|
Type I: Dilatation of extrahepatic biliary tree (60%). |
Type III: Choledochocele—cystic dilatation of intraduodenal part of CBD (5%). |
|
Type Ia—cystic. |
Type IV: Dilatation of extra- and intrahepatic or multiple parts of extrahepatic biliary tree (30%). |
|
Type Ib—focal segmental (saccular). |
Type IVa: Dilatation of extrahepatic and intrahepatic biliary tree. It is 2nd most common. |
|
Type Ic—fusiform. |
Type IVb: Dilatation of multiple sections of the extrahepatic bile duct. |
|
Type II: Diverticulum of extrahepatic biliary tree (5%). |
Type V: Dilatation of the only intrahepatic biliary tree (Caroli’s disease). |
Copyright Preserve, USMCP
Types of Choledochal Cysts (Todani Modification
of Alonso-Lej Classification)
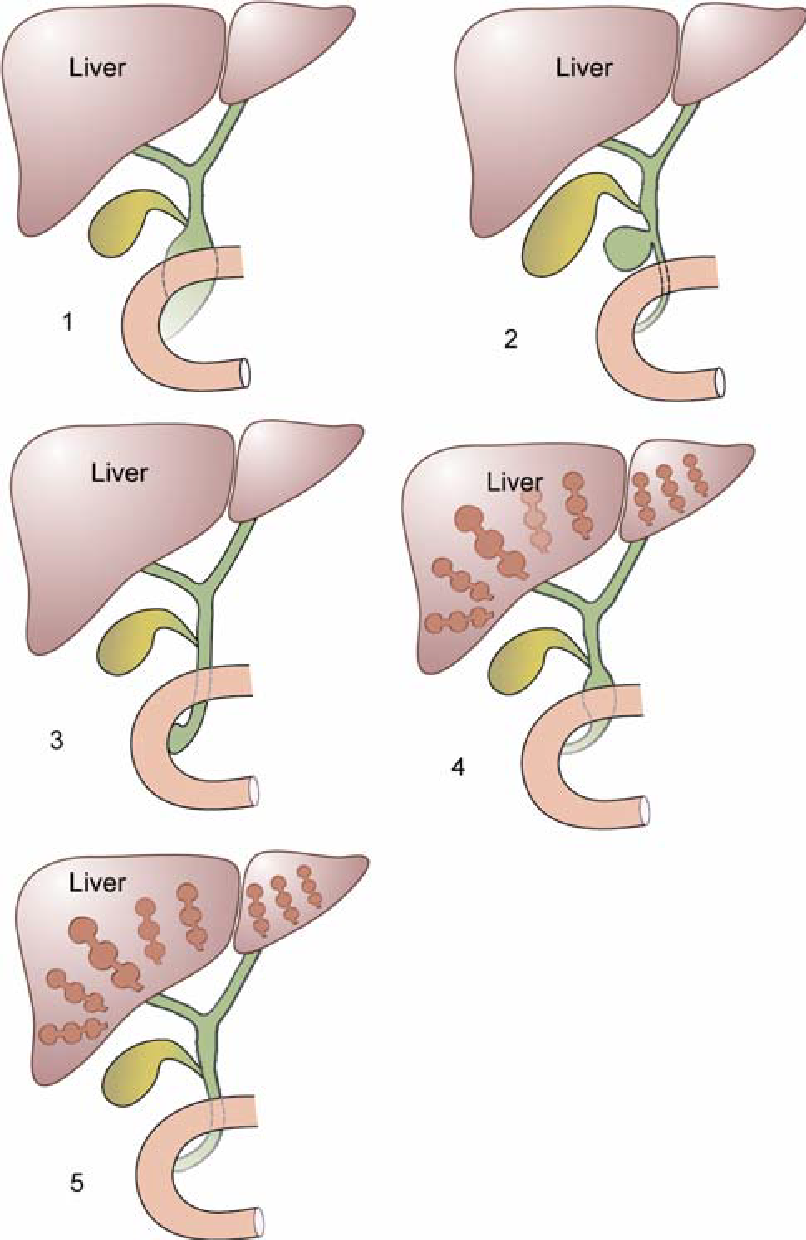
Fig: Different types of choledochal cysts—(1) Fusiform type,(2) Saccular type, (3) Choledochocele,
(4) Fusiform + Intrahepatic type, (5) Intrahepatic type.
Sick Sinus Syndrome
A 16-year-old patient, a native of Connecticut was brought to the ED for symptoms of syncope and dizziness for the past 1 week. Just before the patient was brought, he had a brief episode of syncope without any confusion after the episode. The patient also describes that he has pain in his joints. He also said that he has been to Connecticut 5 weeks back to visit his family and had a fun time with his friends in the woods. When asked about any rashes, he said that he saw a rash approximately 1 week after he came from the trip but didn't notice it that much because it disappeared after some time without any treatment. Apart from these, he doesn't have any other symptoms. Review of systems was normal apart from those described above. Family history is normal and he doesn't drink alcohol, smoke or use recreational drugs. The patient is now alert and oriented. Lung examination is normal and S1, S2 are present. No murmurs. A complete neurologic examination is normal. His vital signs are BP- 90/60, HR- 45/min, RR- 18/min, and Temperature- 36.8C. ECG in the ED is given below.
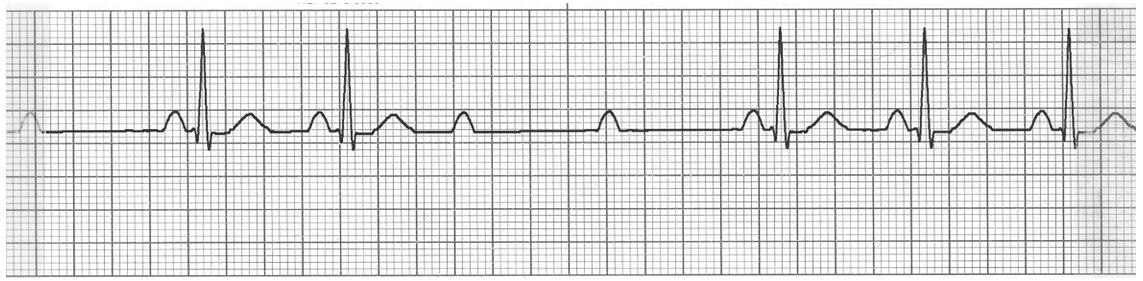
A temporary transcutaneous pacing is tried but without any benefit. During the procedure, he had one more episode of dizziness. What is the next best step for this patient?
A) Observe in the ED and send the patient home
B) Continuous trials of transcutaneous pacing and also get Lyme disease serology.
C) Temporary transvenous pacing and also checking for Lyme disease serology
D) Trial of Atropine
E) Carotid sinus massage
Explanation: The correct answer is C.
The patient with his history of rash, musculoskeletal symptoms, dizziness, and syncope with second degree AV block type 2 on ECG (Similar PR interval followed by blocked sinus P wave and PR interval is same before and after the block) is consistent along with recent travel to woody areas in Connecticut most likely has Early Disseminated Lyme disease. This patient is having symptoms because of his heart block and is temporary because it is caused by Lyme disease. So, the rationale is to start symptomatic treatment, confirm the diagnosis of Lyme disease and start definitive treatment. This patient is having syncope and dizziness with bradycardia and hypotension which if not treated most likely can progress to a complete heart block. So, He should have a trial transcutaneous pacing. But this has been done, failed and the patient had one more episode of syncope. So the next best step is to do a temporary transvenous pacing which will most likely treat his arrhythmia. When the Lyme titers are back, we can start the patient on IV doxycycline followed by oral doxycycline for at least 14-21 days for the early disseminated disease. IV ceftriaxone is generally not preferred for cardiac manifestations of Lyme disease but instead, we can use it for more severe manifestations like Meningitis or Radiculopathy.
(Choice A) Observation and sending the patient home is not correct because this patient has Symptoms like syncope and dizziness and ECG findings showing second degree AV block which will progress into a complete heart block. So, he needs to be treated temporarily with transvenous pacing and also with appropriate antibiotic therapy.
(Choice B) A trial of transcutaneous pacing has been done which didn't treat the arrhythmia and also he had another episode of syncope after that. So, more trials of transcutaneous pacing are not going to work and he needs a transvenous pacing, which will likely bring him back to sinus rhythm.
(Choice D) A trial of atropine is very devastating to the patient as this can worsen second-degree av block type 2. If it was even a type 1, this is not the correct choice as the patient has been having symptoms more often and he needs a definitive treatment for his arrhythmia until he is started on antibiotics.
(Choice E) Carotid sinus massage may improve Second degree AV block type 2 but it is not recommended in this patient because of the above-given reasons.
Educational Objective:
Any patient presenting with Second degree AV block with symptoms should be treated with temporary transcutaneous, if failed then transvenous pacing. At the same time, we should also search for a cause. In patients with history of travel to areas endemic for lyme disease and presenting with AV blocks, Do a Lyme disease serology and treat accompanying symptoms. When the tests come positive, start the patient on appropriate antibiotics. Permanent Pacing is usually not required if a cause has been found. But if there is no apparent cause then permanent pacing is preferred. (Dr. Vemireddy Lalitha - USMCP TEAM)
Coarctation of Aorta
A previously healthy 22 year old college student is brought to the emergency department by his parents after they observed him having severe headaches and vomiting . He described it as the “worst headache of my life”.He has a previous history of recurrent nose bleeds. He has a strong radial pulse; however, his femoral pulse is weak. A chest x-ray was taken. Notching of ribs were noted. An ECG revealed patterns of left ventricular hypertrophy. A neurological examination reveals no focal neurological deficits .Which of the following is the most appropriate immediate step in diagnosis?

-
Echocardiography
-
Plain CT of chest
-
CT Angiogram of chest
-
CT brain
-
Cardiac Catheterization
Explanation: The correct Answer is D:
This patient has the adult type of coarctation of aorta. Especially in the adult form, the individuals suffer from complications of persistent hypertension in the form of aortic rupture or intracranial hemorrhage from an aneurysm of the circle of Willis. This individual especially suffered from a subarachnoid hemorrhage. Therefore, the immediate investigation of choice for this individual is a CT scan of the brain.
(Choice A) An echocardiography is an investigation that can be done for a coarctation of aorta. The echo can reveal the left ventricular functioning as well as provide visualization of the coarctation from the suprasternal notch. However, the immediate emergency in this patient is the subarachnoid hemorrhage rather than the coarctation.
(Choice B) Plain CT scanning of the chest is not the investigation done for coarctation of aorta. MRI is normally done in coronal plane to visualize the coarctation
(Choice C) CT angiography of chest allows for localization and severity of the coarctation. A CT angiogram can also reveal the collateral blood vessels involved such as the intercostal arteries and epigastric arteries. The information gathered from this investigation can be used to determine treatment options for the coarctation, but the immediate concern for the patient is the subarachnoid hemorrhage.
(Choice E) Cardiac catheterization is most often done for symptomatic infants to reveal the left atrial and left ventricular hypertension. This investigation can also reveal the systolic pressure difference between the left ventricle and the femoral artery.
Educational Objective: Patients with adult type coarctation of the aorta at increased risk for ruptured intracranial aneurysms because of the increased incidence of congenital berry aneurysm of the circle of Willis. Even Though a CT angiogram of chest will reveal aortic coarctation, the immediate management should be aimed at SAH for which CT brain is preferred within 6 hours of onset .An MRI scan may be more sensitive than CT after several days. (Dr. Freny Sebastian - USMCP TEAM)
Reference:
Kasper, D. L., & Harrison, T. R. (2005). Harrison's principles of internal medicine. New York: McGraw-Hill, Medical Pub. Division.
Hurst, J.W, Schlant, R.C,& Rackley, C.E. (Eds). (n.d). The Heart (Seventh ed., Vol 1). Newyork City, NY: McGraw-Hill Information Services Company (Health Division)
Paroxysmal Supraventricular Tachycardia (PSVT)
A 20 year old musician comes to the clinic for a regular health check up. He has been healthy until last month when he started to have palpitations. He says that he is worried about his symptoms as it often occurs while he is performing music and has to stop because he feels dizzy. Past medical history is significant for ‘bad sore throat’ when he was a kid but the patient is unable to provide details. His father died at the age of 45 due to some heart disease and his mother is alive and healthy. He admits to using marijuana occasionally but denies any intravenous drug use. He also says he has to take a shot of vodka before every performance which gives him a ‘boost’. His pulse is 94/mins and BP is 122/88 mm hg, respirations are 16/min and temperature is 37.4 C. Cardiovascular examination reveals a I/VI systolic murmur in the pulmonary area. Remaining of the examination is normal. An electrocardiogram is done at the office which is normal. An echocardiogram performed next day does not reveal any abnormality. His blood tests report show the following:
Complete blood count:
Hemoglobin: 12 gm/dl
Hematocrit: 45%
Platelet count: 300,000/mm3
Leukocyte count:
Segmented Neutrophils: 60%
Lymphocytes: 38%
Monocytes: 2%
Serum Chemistry:
Sodium: 145 mEq/L
Potassium: 4 mEq/L
Chloride: 104 mEq/L
Bicarbonate: 24 mEq/L
Serum TSH: 1.2 μU/ml
The physician suspects a paroxysmal arrhythmia which involves a reentry mechanism. Which of the following is the next best step in diagnosing the condition of this patient?
-
Transesophageal Echocardiogram
-
Repeat Electrocardiogram during an episode
-
Electrophysiological studies
-
Chest Radiograph
-
Cardiac Catheter
Explanation: The correct answer is B
This patient most probably has Paroxysmal Supraventricular Tachycardia (PSVT). His symptoms include episodic palpitations and dizziness which seem to be associated with alcohol use. His resting physical and ECG findings are normal which is typically seen in patients with PSVT. PSVT is a one of the Tachyarrhythmias that occurs in paroxysms and the patient is completely asymptomatic in between these episodes. Tachyarrhythmias can be supraventricular or ventricular in origin. Supraventricular tachyarrhythmias are also known as Narrow-Complex tachyarrhythmia (QRS <120 ms) and originate from Atrioventricular Node or anywhere above it while Ventricular tachyarrhythmias (Choice E), also known as Wide-Complex tachyarrhythmia (QRS >120 ms), originate from outside the normal conduction system or has an abnormal His–Purkinje system. PSVT is one of the variants of Supraventricular Tachyarrhythmias which is believed to be due to reentry mechanism in the conduction system in the majority of the cases. Physical exam findings are often normal in these patients with tachycardia as the only sign during an episode. A murmur of I/VI in the pulmonary area may be considered functional(innocent) murmur which is confirmed by a normal echocardiogram.
Workup for PSVT starts with exclusion of organic disorders. Although any patient with cardiac symptoms should undergo an ECG recording, in patients with PSVT, ECG might be completely normal when they are asymptomatic in between episodes. The next best step for diagnosis would be a repeat ECG when the patient is having symptoms (Choice B). A routine blood count may be helpful for screening other disorders. Thyroid abnormalities and electrolyte imbalance can cause arrhythmias, thus ruling them out is necessary. A transthoracic echocardiogram is enough to rule out structural heart disease and a transesophageal echo (Choice A) is not required.
Although Electrophysiological studies (Choice C) are confirmatory and show the exact abnormality in the conduction pathway they should be reserved for later when the diagnosis is uncertain after more simpler tests. A repeat ECG during an episode gives the diagnosis in most of the cases. Chest Radiographs (Choice D) are usually normal in patients with arrhythmia and are not useful. Valvular lesions of the heart may bring about structural changes in the heart after a long time which might be evident in Chest radiographs. Cardiac Catheterization (Choice E) is usually used for chamber pressure studies and interventions. They are certainly very useful in diagnosing valvular heart disease with the help of abnormal pressure gradient but its use in PSVT is therapeutic rather than diagnostic i.e. it may be used for radiofrequency catheter ablation.
Learning Objective:
Paroxysmal Supraventricular Tachycardia can be diagnosed with episodic symptoms and typical ECG findings during an episode. Electrophysiological studies are reserved for later incase of diagnostic dilemma. (Dr. Bishesh Shrestha - USMCP TEAM)
Mitral Regurgitation
A 57-year-old woman with Past medical history of hypertension came for a routine evaluation every 6 months. She generally feels well. She feels all right with routine daily activities such as- walking on flat surfaces or housecleaning. She occasionally had SOB while walking upstairs. She has a past medical history of HTN and she is on Losartan for hypertension and Ranitidine for heart burn. Her mother was hypertensive and social history is noncontributory. On physical examination, no significant findings on HEENT examination, lungs are clear to auscultation, abdomen is soft, nontender and nondistended and there is no peripheral edema. On CVS examination, there is a systolic murmur at the apex and radiating to the axilla. The murmur increased with exhalation and decreased with standing and Valsalva maneuver. Given the clinical scenario, which of the following is the clinical diagnosis?
(A) Aortic Stenosis
(B) Aortic Regurgitation
(C) Mitral Valve Prolapse
(D) Mitral Regurgitation
(E) Mitral Stenosis
Explanation: The Correct Answer is D
This is a case of Mitral Regurgitation as there was a systolic murmur at the apex and radiating to the axilla. The murmur INCREASED with exhalation and DECREASED with standing and Valsalva maneuver. MR is caused by HTN, Heart disease and other conditions that leads to dilation of the heart. Dyspnea on exertion is the most common complaint like the patient in the scenario. The murmur of MR is holosystolic and obscures both S1 and S2. Amyl nitrate also decreases the intensity of the murmur. S3 gallop is often present as well.
(Choice A) This is not a case of Aortic Stenosis as there was a systolic murmur at the apex and radiating to the axilla. The murmur increased with exhalation and decreased with standing and Valsalva maneuver. The murmur of Aortic Stenosis is heard best at the second right intercostal space and radiates to the carotid arteries. It is classically described as a crescendo-decrescendo murmur and it increases with squatting and leg raising and decreases with standing and Valsalva maneuver. (Choice B) The murmur of aortic regurgitation is heard at the lower left sternal border. The murmur increased with squatting and leg raising and decreases with standing and Valsalva maneuver.(Choice C) Mitral Valve prolapse is common in young female and commonly presents with systolic murmur that decreases with squatting and leg raising and increases with standing and Valsalva maneuver.
(Choice E) In Mitral Stenosis, the murmur is a diastolic rumble after an opening snap which can be described as an extra sound in diastole. The S1 is louder. As the mitral stenosis worsens, the opening snap moves closer to S2.
Educational Objective:
The murmur of MR is holosystolic at the apex and radiates to the axilla. The murmur increased with exhalation and decreased with standing and Valsalva maneuver. (Dr. Nadia Hossain - USMCP TEAM)
Pulmonary - Chronic Obstructive Pulmonary Disease (COPD)
1. A 65 years old male retired construction worker comes to the ED with shortness of breath for since the last 4 hours. He has had cough, runny nose and generalized malaise since the last 2 days. Upon taking further history in the ED, the patient says that he has been having frequent cough in the last 5 years with 3 cups full of whitish sputum daily from December to February every year since the last 3 years. He reports that the sputum production has increased in the last 3 days and has become thick yellow with streaks of blood. He also complains of increased difficulty breathing in the same period of time. He has smoked 1 pack of cigarette for the last 25 years. Family history is significant for COPD in his dad under home oxygen therapy and inhaled bronchodilators. He has a BP of 110/60, Respiratory rate of 24/min, Temperature of 101.9 degrees and pulse of 115 per minute. Spo2 at the ED shows 86% in room air. Labs show WBC count of 14,000 with 85% neutrophils, Serum Na of 139 and K of 3.8. Upon examination, he has fine crackles at the left lower lung field with tachycardia and tachypnea. What is the most probable diagnosis in this patient?
-
Adult Onset Asthma
-
A1-anti trypsin deficiency
-
Pulmonary embolism
-
Bronchiectasis
-
Chronic Bronchitis
-
Silicosis
The Correct answer is E
2. What is the best initial test for this patient?
-
Spirometry
-
Chest x ray
-
Blood gas
-
Bronchoscopy
-
Spiral CT
-
D-dimer
-
CT chest
-
Pulmonary Angiogram
-
Skin allergy test
-
PPD
-
Sputm Gm stain and Culture
The Correct answer is B
3. The patient was then started on supplemental oxygen, inhaled bronchodilators, oseltamivir and antibiotics. The patient improved over the next 3 days and he was ready to go home. The attending physician asked him to come for a follow up testing at his clinic. What is the best test to do now?
-
Spirometry
-
Blood gas
-
Spiral CT
-
D-Dimer
-
Pulmonary Angiogram
-
Bronchoscopy
-
Chest x ray
The Correct answer is A ( Dr. Bonas Dahal - USMCP TEAM)
Myocardial Infarction
A 49 year old male arrived in the emergency department complaining of shortness of breath and chest discomfort. The ECG showed ST elevation in V1-V4 and cardiac enzymes showed elevated troponin. An Angioplasty was done on the patient, which relieved the blockage. On the 6th postoperative day, patient is complaining of extreme shortness of breath and substernal chest discomfort radiating to chest and jaw. On physical examination, his PR= 110/min, BP=90/60 mmhg, RR=24/min, clinically afebrile and JVP is raised. What should be the next step in intervention?
-
-
Intravenous normal saline
-
Echocardiography
-
Chest xray
-
Pericardiocentesis
-
Repeat EKG
-
Explanation: The correct Answer is D
The patient came to the emergency department complaining of shortness of breath and chest discomfort and the ECG showed ST elevation in V1-V4 and cardiac enzymes showed elevated troponin. This is indicative of MI for which angioplasty was done. On the 6th postoperative day the patient complained of extreme shortness of breath and substernal chest discomfort radiating to chest and jaw. This along with raised JVP and Hypotension is indicative of cardiac tamponade (also muffled heart sounds = Beck’s Triad) and the patient needs immediate Pericardiocentesis to relieve the pressure.
Cardiac tamponade, also known as pericardial tamponade, is when fluid in the pericardium builds up and results in compression of the heart. Onset may be rapid or more gradual. Symptoms typically include those of cardiogenic shock including shortness of breath, weakness, lightheadedness, and cough. Other symptoms may relate to the underlying cause. Diagnosis may be suspected based on low blood pressure, jugular venous distension, pericardial rub, or quiet heart sounds.
When tamponade results in symptoms, drainage is necessary. This can be done by pericardiocentesis, surgery to create a pericardial window, or a pericardiectomy.
This commonly occurs as a result of chest trauma (both blunt and penetrating), but can also be caused by myocardial rupture, cancer, uremia, pericarditis, or cardiac surgery, and rarely occurs during retrograde aortic dissection, or while the person is taking anticoagulant therapy.
Initial diagnosis can be challenging, as there are a number of differential diagnoses, including tension pneumothorax, and acute heart failure. In a trauma patient presenting with PEA (pulseless electrical activity) in the absence of hypovolemia and tension pneumothorax, the most likely diagnosis is cardiac tamponade.
Tamponade can often be diagnosed radiographically. Echocardiography, which is the diagnostic test of choice, often demonstrates an enlarged pericardium or collapsed ventricles. A large cardiac tamponade will show as an enlarged globular-shaped heart on chest x-ray.
Initial management in hospital is by pericardiocentesis. This involves the insertion of a needle through the skin and into the pericardium and aspirating fluid under ultrasound guidance preferably. This can be done laterally through the intercostal spaces, usually the fifth, or as a subxiphoid approach. A left parasternal approach begins 3 to 5 cm left of the sternum to avoid the left internal mammary artery, in the 5th intercostal space. Often, a cannula is left in place during resuscitation following initial drainage so that the procedure can be performed again if the need arises. If facilities are available, an emergency pericardial window may be performed instead, during which the pericardium is cut open to allow fluid to drain. Following stabilization of the patient, surgery is provided to seal the source of the bleed and mend the pericardium.
(Choice D) is the most appropriate management as emergency pericardiocentesis will relieve the patient’s symptoms.
(Choice A) is good for volume expansion to treat hypotension but the patient also has a raised JVP, in which volume expansion would do more harm than good. It can be done after pericardiocentesis.
(Choices B, C, and C ) will not help relieve the patient's immediate symptoms. These can be additional investigations after the patient has stabilised.
Educational Objective:
Cardiac tamponade is a medical emergency that requires urgent drainage of the pericardial fluid. Preferably, patients should be monitored in an intensive care unit. After pericardiocentesis, the intrapericardial catheter is left in place after securing it to the skin using sterile procedure and attaching it to a closed drainage system via a 3-way stopcock. Reaccumulation of fluid is periodically checked and drained as needed.The catheter can be left in place for 1-2 days and can be used for pericardiocentesis. Serial fluid cell counts can be useful to discover an impending bacterial catheter infection, which could be catastrophic. If the white blood cell (WBC) count rises significantly, the pericardial catheter must be removed immediately. ( Riya Kaur Kalra- USMCP TEAM)
References:
-
Cardiac Tamponade. [Online]. 2017 May 3 [cited 2017 May 20]. Available from: URL: https://en.wikipedia.org/wiki/Cardiac_tamponade#Diagnosis
-
Yarlagadda C. Cadiac Tampnade treatment & management. [Online]. 2016 [cited 2017 May 20]. Available from: URL: http://emedicine.medscape.com/article/152083-treatment
Mitral Valve Prolapse
A 38 year old Male with past medical history of Marfan syndrome comes in for a regular follow up visit to his physician. His main complaint today is shortness of breath upon exertion or climbing 2 flights of stairs, chest pain accompanied with heart racing and easy fatigability. Upon physical examination, the physician notices a late systolic murmur, which was accentuated on standing and deep forceful exhalation. Patient’s previous lab reports were all within normal limit. The physician recommends the patient to do an echocardiography to confirm what could be causing the cardiovascular symptoms. Which of the following is the most likely diagnosis?
-
Myocardial infarction
-
Floppy valve syndrome
-
Endocarditis
-
Mitral regurgitation
-
Atrial septal Defect
Explanation: The correct answer is B.
Floppy valve syndrome, also known as Mitral valve Prolapse (M, is most often associated with Marfan's Syndrome. The patient complains of the above mentioned cardiovascular symptoms. Valsalva maneuver and standing decrease the venous return to the heart, thus decreasing preload. (Choice A is incorrect). MI can lead to papillary dysfunction causing valve prolapse and late systolic click. However, it occurs as an acute condition. (Choice C is incorrect) as the patient has no history of fever and no abnormal blood reports. The blood cultures were negative. (Choice D is incorrect). The patient’s murmur does not radiate to the back or clavicle area as it does with MR. (Dr. Suvi Jain - USMCP TEAM)
Pediatrics - Patent Ductus Arteriosus
A 6-day-old girl has pulmonary congestion. Her mother also mentioned that her newly born baby has serious difficulties in breathing, which cause her problem in feeding. The girl was born at home with the delivery attended by an expert midwife. Physical examination confirms that she is in respiratory distress and shows bounding peripheral pulses with a loud continuous precordial machinery like murmur. X-ray films show increased pulmonary vascular markings. Shortly thereafter, the infant goes into overt heart failure. Which of the following would most likely be required to correct this problem?
(A) Indomethacin
(B) Digitalis and diuretics
(C) Emergency surgical closure of atrial septal defect
(D) Emergency surgical division of patent ductus arteriosus
(E) Emergency surgical closure of ventricular septal defect
Explanation: The correct answer is D.
The diagnosis should be easy to make, since the “machinery-like murmur” is classic for patent ductus arteriosus (PDA). In premature infants who are not in failure, closure can be achieved medically with the use of indomethacin.Non-premature infants are less likely to respond, and infants in overt heart failure cannot wait at all andneed immediate surgical correction. Indomethacin (choice A), as noted above, is ideal for the premature infant who is not in failure. Digitalis and diuretics (choice B) will indeed be used as the infant is rushed to surgery, but, as the question is framed, they alone cannot correct the problem.
The infant does not have either an atrial septal defect (choice C) or a ventricular septal defect (choice E). Neither of those gives a continuous machinery-like murmur or produces bounding peripheral pulses. (Mohammadamin Rezazadehsaatlou - USMCP TEAM)
Amenorrhea
A 29 year old athletic female presented to her gynecologist because of cessation of menses for 26 months. She started having irregular periods and then it completely stopped. For the past 3 years she has been training for a marathon and has been running 10 miles per day. She is 5' 6", weighs 113 Ib and her BMI is 18.1. On physical examination, no hirsutism or galactorrhea is noted. She is sexually active and used an IUD for 4 years. Her β-hCG in urine is negative, serum FSH and LH levels are low and serum prolactin is 15 ng/mL. She also had no withdrawal bleeding after treatment with medroxyprogesterone acetate. What caused her to have amenorrhea?
A. Functional hypothalamic amenorrhea
B. Hypothalamic pituitary dysfunction
C. Polycystic ovary syndrome (PCOS)
D. Due to IUD use
A 65 year old obese female with past medical history of Hypertension presented to the clinic complaining of vaginal spotting occurring 3 to 5 times per month. Her last menstrual period was 14 years ago in which she was taking HRT to control her menopause symptoms for 5 years. Her menstrual periods were heavy and irregular. Her last pelvic exam and pap smear were normal.
A. Ultrasound of the pelvis
B. Endometrial biopsy
C. Colposcopy
D. FSH/LH serum
A 36 year old G3P3 woman presented to the clinic with abnormal heavy menstrual bleeding. She complains of intermenstrual bleeding, dyspareunia and increased pelvic pressure. On pelvic examination, her uterus is enlarged, asymmetric and non-tender. Urine β-hCG is negative. Thyroid stimulating hormone Complete blood cell count reveals the following: WBC 7, hemoglobin 10, Htc 27, and platelets 270. MCV is 69.Transvaginal ultrasound showed hyperechoic, well-circumscribed round mass. What is the most likely diagnosis?
A. Uterine Leiomyomas (fibroids)
B. Endometriosis
C. Adenomyosis
D. Endometrial polyp
(USMCP TEAM)